
High Tibial Osteotomy (HTO)
Authors
Prof Leo Pinczewski MBBS, FRACS
Dr Keran Sundaraj MBBS, MSc (Trauma), FRACS, FAOA
What is an Osteotomy?
An osteotomy is a surgical procedure where a bone is cut and repositioned to correct alignment. In the lower limb, this is commonly performed on the proximal tibia (upper shin bone, just below the knee) or distal femur (lower thigh bone, just above the knee). The goal is to correct bow-legged (varus) or knock-kneed (valgus) alignment, shifting the body’s weight away from worn or arthritic parts of the knee joint. This joint-preserving procedure helps relieve pain, improve function, and may delay or prevent a total knee replacement in younger or active patients.
Why Is a Knee Osteotomy Performed?
Knee osteotomy is most often recommended for patients with unicompartmental osteoarthritis (arthritis in just one part of the knee), especially when the leg is misaligned. For example, bow-legged patients often wear out the medial (inner) side of the knee. An osteotomy straightens the leg to offload this damaged area, redistributing pressure to the healthier lateral (outer) compartment.
This procedure is particularly effective for younger patients under 55, those who are active, and those with good remaining cartilage in the unaffected compartment. In these cases, osteotomy can delay the need for knee replacement by 10–20 years.
Studies from our clinic show a 91% success rate at 5 years, 80% at 10 years, and 60% at 20 years in well-selected patients. Importantly, having had an osteotomy does not prevent future knee replacement if needed.
Understanding Knee Alignment
In a normally aligned leg, a straight line from the hip to the ankle passes through the center of the knee. In a varus (bow-legged) leg, this line shifts inward, increasing stress on the medial compartment. In valgus (knock-kneed) legs, the line shifts outward, overloading the lateral compartment.
Osteotomy adjusts this alignment:
For varus (bow-legged): the goal is to realign the leg into mild valgus, relieving medial pressure.
For valgus (knock-kneed): the goal is to shift the leg toward neutral, offloading the lateral compartment.
A/Prof Sundaraj carefully plans each correction with computer modelling and 3D printed cutting guides to ensure optimal alignment and knee function.
Osteotomy Techniques
There are three main types:
Closing Wedge: A wedge of bone is removed, and the bone edges are closed together.
Opening Wedge: The bone is cut and wedged open, with a gap filled using bone graft.
Dome Osteotomy: A curved cut allows rotation around a central axis without removing bone.
The technique used depends on your anatomy, deformity, and specific surgical goals. Below are more details:
Closing Wedge Osteotomy
A small triangular wedge of bone is removed. For varus correction, this is done on the lateral tibia; for valgus correction, on the medial femur. The remaining bone edges are closed and fixed with a plate and screws.
Leg becomes slightly shorter (a few millimetres).
Often requires a fibular osteotomy.
Reliable healing due to large bone contact area.
May be more technically challenging for future knee replacement—but manageable with robotic assistance.
Opening Wedge Osteotomy
Instead of removing bone, a cut is made and gently opened to the desired angle. The wedge-shaped gap is stabilized with a plate and often filled with bone graft or substitute.
Leg may become slightly longer (a few millimetres).
No need to cut the fibula.
Allows precise adjustment during surgery.
Slightly higher risk of delayed bone healing or non-union.Dome Osteotomy
A curved cut (dome) allows the bone to rotate around its center without removing or adding length.
Leg length is more closely preserved.
Useful for complex deformities but technically more challenging.
Avoids changing joint slope or patella height.
Less commonly used but valuable in selected cases.

(A) In a normally aligned leg, the weight-bearing axis (dotted line) runs through the centre of the hip, knee and ankle. (B) With a varus (bow-legged) deformity, the weight-bearing axis runs through the centre of the hip and ankle, but through the diseased medial side of the knee. (C) A lateral closing wedge high tibial osteotomy removes a wedge of bone from the lateral side of the proximal tibia. (D) Post-osteotomy the leg is aligned in an appropriately over-corrected valgus (knock-kneed) position and the healthy lateral compartment takes the majority of the load. This relieves the pain and gives the medial compartment a chance to heal.
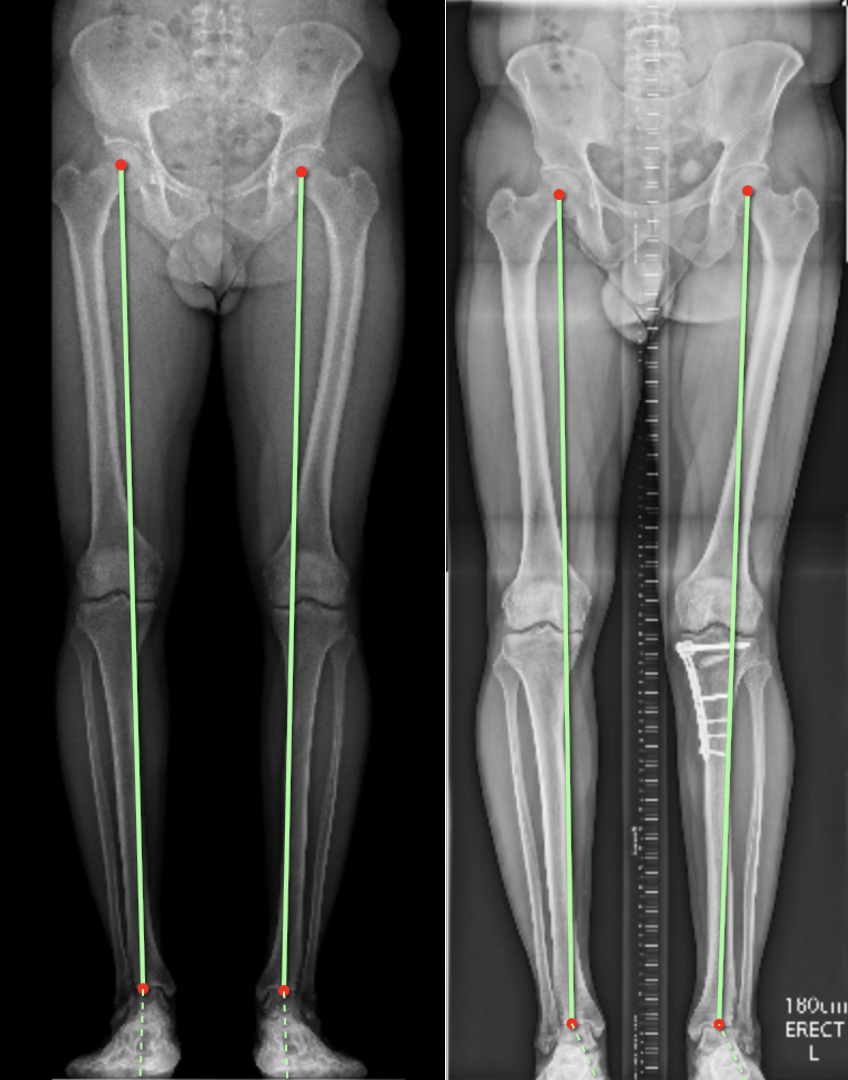
The picture on the left shows the weight-bearing axis passing through the inner (medial joint). The picture on the right is the same patient after surgery. A medial opening wedge high tibial osteotomy was performed with bone grafting. Post-osteotomy the leg is aligned in an appropriately over-corrected valgus (knock-kneed) position and the healthy lateral compartment takes the majority of the load.

A medial opening wedge high-tibial osteotomy with artificial bone graft.
Success Rates and Outcomes
Most patients report significant pain relief and improved mobility within 3–6 months. While osteotomy does not "cure" arthritis, it effectively delays progression and buys time with your native joint.
Ideal candidates (younger, lower BMI, good range of motion) can expect excellent long-term results.
10-year survival: ~80%
20-year survival: ~60% in optimal patients
· 95% patient satisfaction reported in long-term studies from NSORG.
Whether done in the tibia or femur, osteotomy is highly effective in improving function and postponing knee replacement.
Risks and Complications
Complications are uncommon but include:
Cosmetic changes: Leg shape will change and may look different to the opposite leg.
Under- or over-correction: May lead to persistent or recurrent pain.
Leg length discrepancy: Minor length changes may occur (shorter with closing wedge, longer with opening wedge).
Bone non-union: Rare (~2–5%). Bone grafts are used if needed.
Infection: <3%. Usually superficial, managed with antibiotics. For deep infections multiple surgeries may be required.
DVT/PE: Blood clot risk is minimized with blood thinners and early mobilisation.
Nerve injury: Particularly to the peroneal nerve – which may cause a ‘foot drop’. This is rare, but a significant complication
Arterial injury: a very rare but very devastating complications which may lead to amputation
Knee stiffness: Managed with early physiotherapy.
Patella height change: May cause minor issues with squatting or kneeling.
Hardware irritation: Some patients elect plate removal after healing (~10–20%).
Recovery and Follow-Up
Hospital stay: 1–3 nights.
Weight-bearing: Depends on fixation and bone quality (can range from immediate to 6 weeks non-weight-bearing).
Bracing: Rarely used in A/Prof Sundaraj’s protocol.
Wound check: Via photo at 2 weeks.
Medications: Pain relief (paracetamol, NSAIDs and opiates) and short-term blood thinners.
Physiotherapy: Begins Day 1 with range of motion, muscle activation, and walking training.
Full recovery: 3–6 months. Return to desk work in 3–6 weeks.
High-impact sports: Delayed or avoided long-term.
Driving: Generally from 6 weeks (right leg); sooner if left leg and driving automatic.
Hardware removal: Optional after 12–18 months if plates cause symptoms.
Osteotomy of the lower limb is a safe and effective surgery that realigns the leg, offloads the worn part of the knee, and delays the need for replacement. With the right patient selection and expert technique, it can keep you active, mobile, and pain-free for many years.
As with all operations, if at any stage anything seems amiss, it is better to call for advice rather than wait and worry. A fever, redness or swelling around the line of the wound or an unexplained increase in pain should all be brought to the surgeon's attention. You can contact Dr Sundaraj by telephoning his staff during business hours or the Mater Hospital after hours. For any questions, please do not hesitate to contact our staff (02) 9437 5999 For after-hour assistance contact Mater Hospital (02) 9900 7300 Further information is available on our website
Get in touch.
Fill out the form and one of the team will be back in touch within 24 hours.
Alternatively, give us a call on
(02) 9437 5999